FIRST, DO NO HARM
/How the harms of PSA testing have been minimised. And how Focal Therapy could reduce them further.

Hippocrates didn’t come up with the term Primum Non Nocere, but his own words are similar.
It’s been nearly 5 years now since our last blog post on Focal Therapy for prostate cancer. But it’s time to revisit this topic, especially now there is a welcome awareness of harm minimisation. Let me explain.
Treating the aggressive forms of prostate cancer is most likely to be curative when it’s still contained within the prostate gland because it can be either surgically removed (radical prostatectomy) or destroyed with radiotherapy. The PSA (Prostate Specific Antigen) blood test is what we’ve used for decades now to help detect prostate cancer before it has spread and become incurable. Like ovarian cancer in women, waiting for symptoms to arise leaves it too late. (Note: urinary symptoms are common in older men, but not because of prostate cancer. They’re caused by benign enlargement of the gland, which restricts the bladder outlet. For prostate cancer to cause urinary symptoms, it has to be advanced because in its early stages, it invades and replaces normal prostate tissue, rather than enlarging the prostate.)
So PSA testing all sounds very sensible and desirable. Yet it has been racked by controversy because it has also led to overdiagnosis and overtreatment of the non-aggressive forms of prostate cancer that may have caused the patient no ill-health at all – let alone caused death.
How did this happen?
When a PSA level is above normal (normal range is 0 – 3.0), it means there’s something going on in the prostate. But it may not be cancer. More often it just means there’s benign (non-cancerous) growth, which is very common in men from their 50s onwards. So although PSA is indeed Prostate-Specific, it’s not Prostate Cancer-Specific. In the past, to help us work out whether an elevated PSA was due to cancer or not, patients would undergo a prostate biopsy (needle sampling of prostate tissue). The problem was that this was an invasive procedure, and when performed via the rectum, also carried a risk of septicaemia (bacterial blood poisoning). And being a random sampling of the prostate, the biopsy would often find the low risk forms of prostate cancer that wouldn’t need treatment. But because it was still the c-word, it would cause the patient untold anxiety. Sometimes, to alleviate both the patient’s anxiety and the concern of their specialist, the patient would undergo treatment anyway. The problem is that traditional curative treatments of prostate cancer treat the whole prostate gland and often cause side effects that have a major impact on quality of life, such as erectile dysfunction and urinary incontinence.
So we had a situation where the treatment was often worse than the disease itself! And all initiated through a simple PSA blood test that led to more harm than good in these cases.
But in the last 8 years, there have been 3 major changes in how we go about diagnosing prostate cancer that have reduced the risks of PSA testing enormously – and a fourth major advance appears to be on its way.
1 MRI

The circled area in the middle image shows the only cancer. The rest of the prostate is normal.
If a PSA level is elevated, rather than biopsy, now the next standard step in finding out if a harmful type of prostate cancer is present is the non-invasive test of a prostate MRI. This scan is extremely helpful in a couple ways. If it shows no cancer, we can usually avoid an invasive biopsy altogether. If it does show cancer, it’s usually a type that has aggressive features. In other words, MRI tends to not see low grade cancers, which are not harmful* – exactly the ones we don’t need to find. When the MRI is positive, we can then perform a biopsy that pinpoints the tumour to ensure maximal diagnostic accuracy. This is important because the biopsy doesn’t just tell us if it’s really cancer, it also tells us how aggressive it is (the grade), which is critical to advising patients on treatment options and prognosis.
*There is currently a hot debate in progress on whether the low grade prostate cancers should even be called “cancer”, or should instead be given another term that doesn’t strike fear into patients’ hearts and interfere with rational decision-making.
2 Transperineal Biopsy
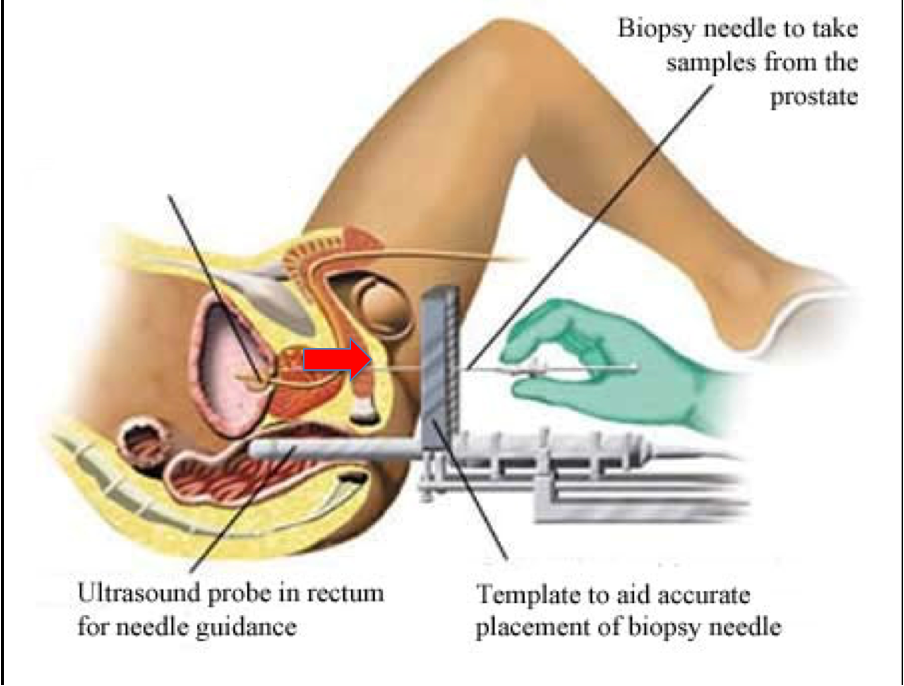
the ultrasound probe sits in the rectum, but the rectal wall is not punctured.
Biopsy used to be performed routinely via the rectum. As mentioned, this meant a risk of septicaemia, due to bacteria being introduced from the rectum into the bloodstream via the biopsy needle. But a biopsy can also be performed by passing the needle via the skin of the perineum (between the scrotum and anus), which is easy to disinfect, so the rate of severe infection is near-zero. Our own research, as well as that of many other groups, has shown this. So if an MRI does show a tumour, the biopsy that follows is now much safer.
3 Active surveillance
In the past, when our diagnostic techniques were so inaccurate, it made some sense that even the low grade cancers were treated with radical prostatectomy or radiotherapy. The reasoning was that these cancers might indicate a higher grade cancer elsewhere in the prostate. Unfortunately, it meant that many patients were treated unnecessarily, leaving them with a worse quality of life. Now that we can see prostate cancer on imaging and target it with a safer biopsy technique, we can be far more confident we’re not missing anything. Occasionally, even though MRI tends to not see the low grade cancers, we may still find them. But the good news is, we know that these cancers are not themselves harmful and so can be safely observed without any treatment at all – what we call Active Surveillance. This involves further PSA testing and imaging and possibly a repeat biopsy down the track, but only if the tumour becomes more aggressive (is upgraded) might we consider switching to curative treatment.
All three of the above measures that minimise harm from initial PSA testing are now evidence-based standard of care. This fourth advance is not. But it appears likely to be in the near future as longer-term data come in.
4 Focal Therapy

MRI shows the cancer. Biopsy confirms and excludes other cancer. Focal therapy is targeted to the cancer accordingly.
What is focal therapy for prostate cancer?
In a nutshell, it’s treatment of just the cancer, not the entire prostate gland, with the aim of curing the cancer while preserving function of all the surrounding structures which are so important for normal function – the erectile nerves, bladder, rectum and urinary sphincter. A classic analogy for this is the lumpectomy for early breast cancer. First considered heretical in the world of cancer surgery, it has been evidence-based standard of care for decades now.
Although technically possible, focal therapy for prostate cancer is not done by surgical resection of the tumour due to the significant anatomical challenge. Instead, the cancer is destroyed by using one of a variety of energy sources that are lethal to cancer cells. These include the traditional modality of brachytherapy (radiotherapy by implanting radioactive seeds, but only into the cancer) which irradiates the cancer, irreversible electroporation (IRE, or NanoKnife) which electrocutes it, HIFU (high intensity focused ultrasound) or laser which heat it, or cryotherapy which freezes it. We don’t yet know which of these types of focal therapy will be the best. And it may be that one modality will be better than another depending on factors like tumour location or size. But focal brachytherapy and IRE use the familiar transperineal approach – the same as modern biopsy techniques.
Early data are mainly useful for testing functional outcomes, that is, side effects on urinary, sexual and bowel function. Not surprisingly, when the surrounding structures that provide these functions are preserved, we’ve found that side effects are kept extremely low. What we continue to wait for are the long-term cancer outcomes, which we expect to come in over the next few years. The hope is that cancer cure or control rates are equivalent to patients with the same type of prostate cancer who have undergone traditional radical treatment. If this bears out, focal therapy would become a fourth major advance in reducing harms in testing for early detection of prostate cancer. Until then, patients who choose focal therapy should be aware that long-term outcomes remain unknown and should have their treatment within a clinical trial or registry so their data can be used to inform optimal treatment in the future.